Artificial Pancreas for Closed Loop Blood Glucose Control
Faculty: Radhakant Padhi (AE) S. Raha (CDS)
Motivation
Diabetes is a long-term disease during which the body’s production and use of insulin are impaired, causing glucose concentration level to increase in the bloodstream. The normal blood glucose concentration level in a human is in the narrow range of 70–110mg/dl. Keeping blood glucose levels as close to normal as possible leads to a substantial decrease in long-term complications of diabetes. A higher value as well as a lower value can lead to a serious illness in human beings. A higher blood sugar level leads to hyperglycemia, whereas a low blood sugar level results in hypoglycemia. Hyperglycemia in the long run can create problems such as stroke, cardiac arrest, blindness, etc. Hypoglycemia (less than 50mg/dl of blood sugar concentration), on the other hand, has more serious consequence as it can rapidly lead to brain failure and hence death of the patient.
Type-1 diabetes presents mainly in children but can occur in adults as well. There is almost no production of insulin and the patients depend entirely on insulin delivered from outside for the blood glucose control. Study shows that the number of patients with good glycemic control is less than 20 percent in type 1 diabetes patients. There is ample evidence to show that a good glycemic control is the only way to avoid or prevent complications of diabetes. This definitely shows that there is need for better management of diabetes, especially in Type-1 patients.
The delivery of insulin today is in the form of insulin injections given prior to meals as a bolus and basal insulin delivery system, which can be in the form of insulin syringes or, by the use of pens. The currently available insulin pumps are an open system where the blood glucose has to be measured and then the pump programmed to give a bolus and basal insulin. The bolus has to be manually metered in depending on the diet physical activity etc. Obviously such an approach can be grossly erroneous and can never be customized to individual patients. Hence, there is a need for a closed loop insulin delivery system (based on closed loop feedback automatic control theory), which should be able to inject the amount of insulin required at a given point of time based on the measured blood glucose level at that point of time. Such a system should also preferably be ‘adaptive’, which can customize the dose not only based on the measured blood glucose level, but also the patients parameters such as the height and weight of the patient, his/her physical activity and other metabolic parameters.
This is the key aim of this research. The concept can be understood from the following illustrative picture (see Ref.1)
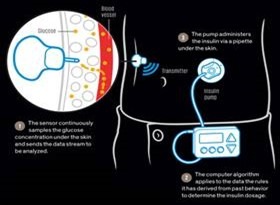
Reference: P. E. Ross, Diabetes Has a New Enemy: Robo-Pancreas. IEEE Spectrum, June 2015
There is a lot of interest worldwide (especially in the US, Europe and Australia) to develop a fairly good artificial pancreas over last 10 years. However, most of the development so far has relies on too simplified control logic such as the standard PID control, fuzzy logic control etc., primarily not to rely too much on the mathematical model of the metabolic process. However, such approaches are obviously not very powerful and can even potentially lead to the danger of over-dosing and hence hypoglycemia. Researches are also being carried out using advanced “model predictive control” theory. However, this approach relies heavily on the predicted behavior of blood glucose over a finite time into the future and hence relies heavily on a good fit of the model to the actual patient. Unfortunately, however, the parameters of the available models are based on trials predominantly of Caucasian population and hence are not expected to work satisfactorily for South-Asian population in general and Indian population in particular.
Hence the primary aim of this project is to:
- Customize the available model by re-fitting the parameters based on experiments over the Indian population (experiments are being done by a separate group in MSR Medical)
- Incorporate advanced nonlinear, adaptive and optimal feedback control theory based algorithms for insulin dosage computation.
- Make the above algorithm operate on closed loop with minimal sensors, by incorporating a Kalman filter for state estimation (there by filtering out the process and sensor noises as well). Note that this can also lead to ‘soft sensing’, which can increase the life of the sensors in the loop (thereby minimizing cost and inconvenience).
The ultimate aim of this research is to develop a life-saving health-care product with is quite advanced and sufficiently cheap for mass consumption and to market the product subsequently. Note that the proposed research will look into many other variables that can possibly impact the glucose regulation in high-fidelity in-silico simulation studies before going for field trials. The variables of interest are meals with different carbohydrate content, exercise and physical activity, physiological changes like menstrual cycle, pregnancy, menopause, inter-current illnesses etc. It can be mentioned here that the other main confounder is of course the hypo-glycaemia (i.e. very low blood glucose level). Hence, there is a need to make an artificial pancreas operate both on insulin as well as glucagon. However, due to practical difficulties and occasional (rare) necessity, glucagon based artificial pancreas will not be considered in this research, which is in tune with the research being carried out world-wide.
Background Needed: Numerical Methods / Optimization / Control Systems / State Estimation (any two will do)